
From Five to Zero: Why This ICU CAUTI Pilot Should Change How We Protect Foley Catheters
Medical Device Distribution, Biologic distribution and Mobile Physician-led Wound Care
January 12, 2026
In healthcare, we often speak about evidence-based practice. What we speak less about is what happens when the evidence is simple, the signal is strong, and the outcome is unambiguous.
That is exactly what occurred in a recent ICU pilot evaluating SpigotGuard (SG), a passive disinfection device designed to protect Foley catheter urinary drainage ports.
The Results Speak for Themselves
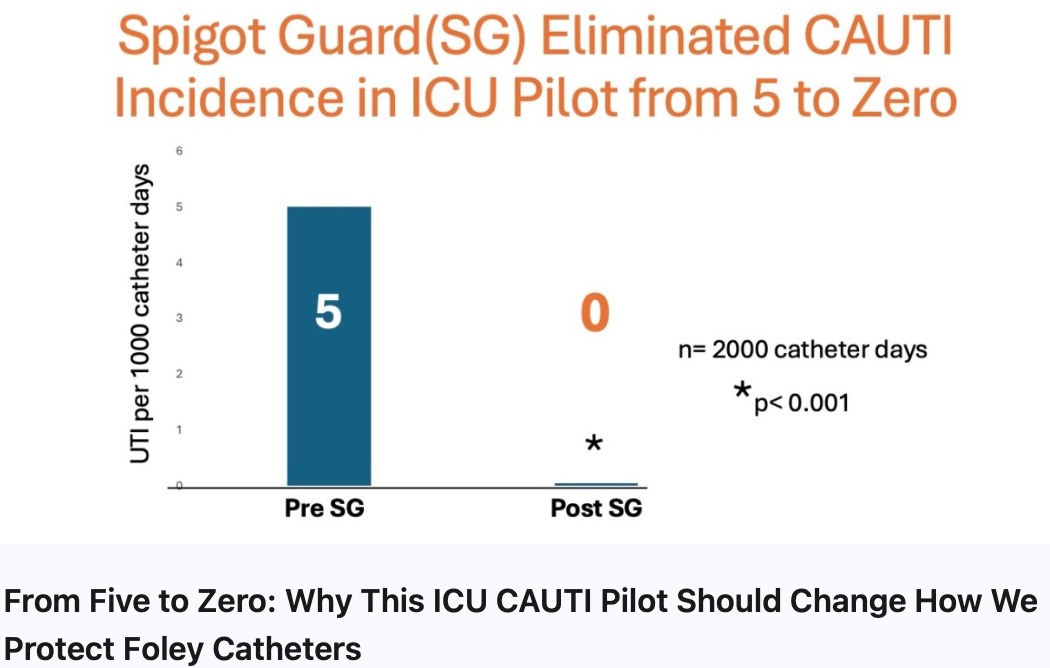
In this ICU pilot, led by Dr. Kelly Hiatt, MD¹, CAUTI incidence declined from 5 per 1,000 catheter-days to zerofollowing implementation of SpigotGuard.
Pre-SG: 5 CAUTIs per 1,000 catheter-days
Post-SG: 0 CAUTIs per 1,000 catheter-days
n = 2,000 catheter-days
p < 0.001
There was no major workflow redesign. No staffing increase. No additional documentation burden. The intervention was passive, always in place, and aligned with standard nursing practice.
The full manuscript detailing the study design, methodology, and statistical analysis is currently being finalized. However, the outcome during the post-implementation period is already clear: CAUTI events were eliminated.
Real-World Evidence vs. Controlled Studies
Randomized controlled trials remain the gold standard of clinical evidence. But infection prevention leaders, nursing administrators, and hospital executives understand an important reality:
Controlled studies demonstrate possibility. Real-world pilots demonstrate adoptability.
This pilot reflects the conditions hospitals actually operate under:
Real ICU workflows
Real nurse-to-patient ratios
Real-world compliance variability
Despite these variables, the outcome was complete CAUTI elimination during the observation period.
This distinction matters. Many interventions perform well under tightly controlled conditions but falter in everyday clinical environments. Passive interventions that reduce reliance on perfect human behavior consistently outperform more complex or behavior-dependent solutions.
Why These Results Parallel the Curos® Cap Adoption Curve
For those familiar with infection prevention history, this pattern should feel familiar.
Early pilot studies of Curos® caps demonstrated dramatic reductions in central line–associated bloodstream infections (CLABSI). Initial skepticism followed—results seemed “too good.” But hospitals soon recognized the common denominator behind the success:
Passive, always-on protection of the access point.
Curos caps did not succeed because they were innovative. They succeeded because they removed uncertainty.
Today, Curos caps are widely considered a standard of care.
SpigotGuard addresses the same vulnerability in Foley catheters that Curos addressed in central lines: the access point.
Foley drainage ports are frequently manipulated
Each access event introduces contamination risk
Manual disinfection is variable and error-prone
By passively protecting the drainage port, SpigotGuard mitigates this risk without adding complexity or burden to nursing workflows.
The ROI Case: Compelling and Conservative
From a financial perspective, CAUTIs are among the most punishing hospital-acquired conditions:
Often unreimbursed
Associated with increased length of stay
Linked to downstream complications and antibiotic exposure
Elevate audit, compliance, and quality-reporting risk
Even conservative financial modeling demonstrates that:
Preventing a single CAUTI can offset the cost of broad device deployment
Scaled implementation yields rapid payback
Cost avoidance is immediate and measurable
This is not speculative revenue generation. It is loss prevention—the most reliable form of margin protection in today’s healthcare environment.
Why This Should Become the Standard of Care
When an intervention:
Eliminates events rather than marginally reducing them
Is passive and workflow-neutral
Mirrors prior successful infection prevention adoption models
Demonstrates a compelling ROI
The question is no longer “Does it work?” The question becomes “Why would we accept preventable harm without it?”
SpigotGuard appears to represent the same inflection point for Foley catheter care that Curos represented for central line protection.
Final Thought
Healthcare does not need more complex solutions. It needs simple ones that work—every time, under real clinical conditions.
This ICU pilot suggests SpigotGuard may be one of them.
John F. Curtis IV, MD
General Surgeon & Medical Consultant
www.spigotguards.com
Chief Medical Director
www.PhiladelphiaWoundCare.com
¹ Dr. Kelly Hiatt, MD — Board-certified Otolaryngologist (Head & Neck Surgery) with ICU clinical leadership experience, practicing in Indianapolis, Indiana; principal investigator for the SpigotGuard ICU CAUTI pilot.
#HospitalAdministration #NursingLeadership #InfectionPrevention #PatientSafety #QualityImprovement #CAUTI #ICUQuality #ValueBasedCare #HealthcareROI #StandardOfCare